A lot of people walk out of their diabetes appointment knowing one number. Their HbA1c. It came back okay, or it came back a little high, and that feels like the whole story for another three months.
But diabetes is not a one-number condition. It affects your eyes, your kidneys, your nerves, your circulation, and your heart, often quietly, often for years before anything feels obviously wrong. Comprehensive diabetes care is the approach that looks at all of it, not just the number that is easiest to track.
If your diabetes visits mostly feel like a quick lab review and a refill, this is worth reading.
Key Takeaways
- HbA1c is a starting point, not the full picture of your diabetes health
- CGM for type 2 diabetes shows blood sugar patterns your meter never could
- Diabetes and poor circulation often develop silently, especially in the feet
- Diabetes and vision loss can progress without any symptoms until damage is done
- Diabetes self-management between visits matters as much as the visit itself
Why One Test Cannot Tell the Full Story
The HbA1c gives your doctor a useful average. It reflects roughly how your blood sugar has been behaving over the past two to three months. That information matters. But averages hide things.
Your blood sugar could be swinging dramatically, going very high after meals and very low at other times, and your HbA1c could still look acceptable. You would not know that from the number alone. And those swings, over time, are doing damage to the same tissues that steady high blood sugar damage.
That is why comprehensive diabetes care involves more than checking the average. It looks at how your blood sugar moves throughout the day, how your organs are holding up under the ongoing pressure, and what warning signs, if any, are starting to appear.
CGM for Type 2 Diabetes and What It Changes
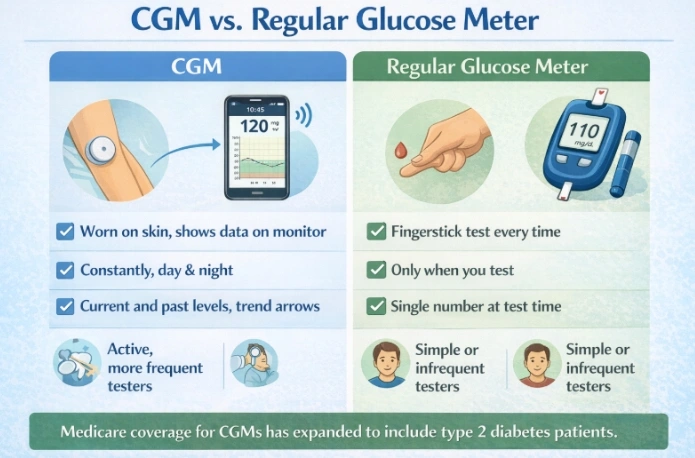
For a long time, continuous glucose monitoring was mostly associated with type 1 diabetes. That has shifted considerably. CGM for type 2 diabetes is now being used much more broadly, and the reason is simple. It tells you things that finger-stick testing cannot.
A continuous glucose monitor sits on your skin, usually on your arm or abdomen, and tracks your glucose levels throughout the day and night. Instead of a single snapshot when you test, you get a running picture. That meal you just ate? Two hours later, you can actually watch what it did to your blood sugar. Overnight drops that used to go completely unnoticed now show up right on your screen. Patterns that would have taken you months to piece together on your own become obvious within days.
For people managing type 2 diabetes through diet, exercise, and medication, that kind of feedback changes things practically. When you can see that your blood sugar spikes sharply after a certain food you thought was fine, you start making different choices. When you can see that your evening walk actually brings your numbers down meaningfully, that is motivating in a way that quarterly lab results simply are not.
Does Medicare Cover CGM for Type 2 Diabetes
This is one of the questions that comes up most often, and the answer has gotten better in recent years. Does Medicare cover CGM for type 2 diabetes? Yes, in many cases it does.
Medicare actually expanded CGM coverage for people with type 2 diabetes who are not on insulin. Your doctor does need to document a few things to make it happen. That includes confirming your diabetes diagnosis, showing that you are on a qualifying medication, and making the case that a CGM genuinely fits your situation medically. It is not complicated, just a conversation worth having at your next visit.
Coverage rules do change and vary by plan, so the most accurate thing to do is confirm the current criteria with your care team or contact Medicare directly. The point is that cost is no longer automatically a barrier to the way it once was, and if you have been assuming CGM is out of reach, it is worth asking.
Blood Glucose Meter Accuracy and Why It Matters
Not every glucose meter performs the same way. Blood glucose meter accuracy varies more than most patients realize, and using a meter that reads consistently off can quietly affect your medication decisions, your dietary choices, and your sense of whether your management is working.
The FDA requires home glucose meters to fall within 15 percent of a lab result at least 95 percent of the time. That sounds reassuring until you realize a 15 percent margin at a blood sugar of 200 means you’re reading could be anywhere from 170 to 230. At the extremes, those differences matter.
Blood glucose meters comparison accuracy studies have found real differences between devices. Test strip quality, storage, expiration, finger site, technique, altitude, and conditions like anemia can all pull your reading away from your actual blood sugar number.
A few things are worth knowing. Store strips in a cool, dry place and never use expired ones. Clean your hands before testing, not just wipe them. If your readings seem inconsistent or do not match how you feel, bring your meter to your next appointment. Many clinics will run a comparison test against a lab to draw, so you can see how accurate your device is.
Diabetes Self-Management Day to Day
Between appointments, diabetes self-management is where most of the real work happens. What you eat, how much you move, whether you take your medications consistently, how you respond to stress, and how well you sleep. All of it feeds back into your numbers and your long-term health.
That can feel a lot of pressure. And the truth is that nobody manages diabetes perfectly every single day. Life gets in the way. Routines break down. Stress raises blood sugar in ways that you feel completely out of control.
What actually works, based on what research and patients consistently report, is not perfection. It is consistency in the basics, the ability to get back on track after a rough stretch and having a care team that helps you understand what your numbers and symptoms are telling you rather than just reacting to them.
Diabetes self-management also means knowing when something has changed. New symptoms deserve attention. Tingling or numbness that was not there before. A cut on your foot that is not healing the way it should. Vision that seems different. These are not things to wait out.
Can Diabetes Cause Vision Loss
Yes, diabetes can cause vision loss. But the more important question is whether you can prevent it, and the answer to that one is also yes.
Diabetes affects small blood vessels throughout the body. In the eyes, those vessels are particularly delicate. When blood sugar stays high over time, those vessels can swell, leak, or grow abnormally inside the eye. That process is called diabetic retinopathy, and it is the leading cause of new vision loss in adults.
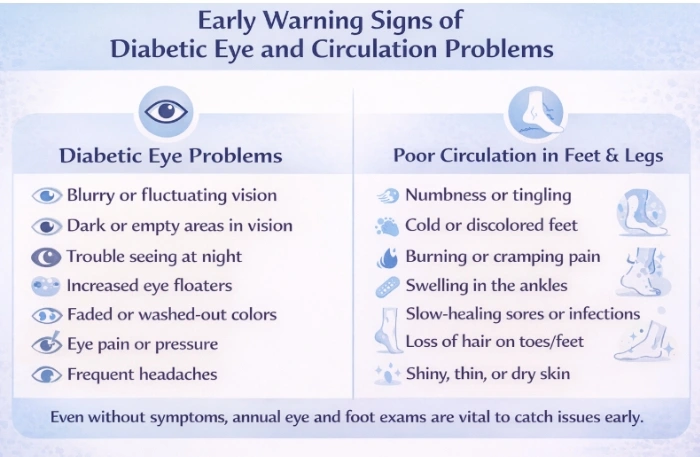
Diabetes and vision loss do not always arrive with obvious warning signs. In the early stages of retinopathy, you may not notice any change in how well you see. By the time vision becomes noticeably blurry or distorted, significant damage may already have occurred.
Annual dilated eye exams catch changes before they turn into actual vision loss. Catching retinopathy early gives your eye doctor real options, laser treatment and injections can genuinely slow it down or stop it from getting worse. None of that is possible if the exam never happens.
Controlling blood sugar, blood pressure, and cholesterol all reduce the rate at which retinopathy progresses. Focusing on one number will never show you the full picture. Comprehensive diabetes care looks at everything, and that wider view is exactly what catches the things glucose management alone will miss.
Diabetes and Poor Circulation
Diabetes and poor circulation tend to develop slowly, which is part of why they go unnoticed for a long time. The same process that damages blood vessels in the eye damages larger vessels throughout the body, particularly in the legs and feet.
Diabetes and poor blood circulation reduce the amount of blood reaching the tissues at the end of the line, your feet. When blood flow is reduced, those tissues get less oxygen and heal more slowly when injured. A small cut or blister that would be minor for most people can become a serious wound for someone with diabetic circulation problems.
Symptoms worth knowing include a feeling of coldness in the feet or lower legs, cramping in the calves when walking that goes away with rest, slow-healing sores, skin that looks shiny or feels tight on the lower legs, and hair loss on the feet or ankles. Any of these deserve a conversation with your doctor.
Circulation problems in the legs and feet are also connected to neuropathy. When you have both reduced circulation and reduced nerve sensation in the same area, injuries can occur and go unnoticed. That is the combination that leads to more serious outcomes. Checking your feet every day, wearing properly fitting shoes, and keeping your toenails trimmed are simple habits with real preventive value.
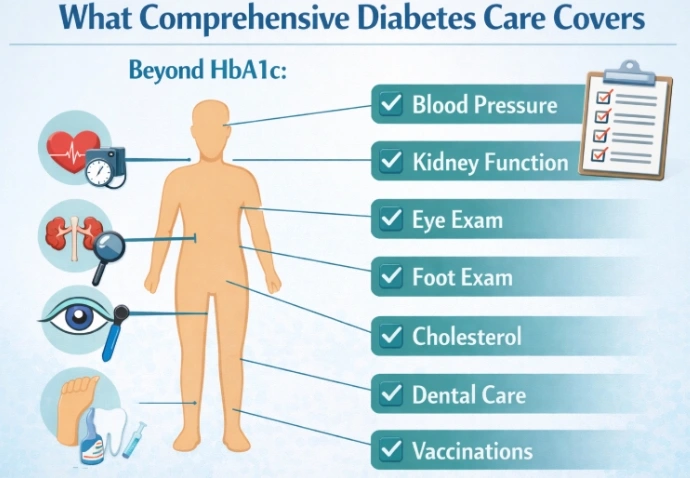
A lot more than just your HbA1c number. Think of blood pressure, cholesterol, kidney function, a proper foot exam, and a yearly dilated eye exam. Your medications should be reviewed regularly, too. And honestly, your doctor should be asking how life is going, not just reading off your latest results and sending you home.
That really depends on you. Your insurance, your daily routine, and what your doctor thinks makes sense for where you are right now with your management. There is no device that works best for everyone. What actually matters is that you use it consistently and pay attention to what the patterns are telling you.
Your primary care doctor is genuinely the best place to start. At Peoples Medical Care McKinney, Dr. Zulfarah Ishaque and Dr. Munaza Gohar work through this with their patients directly, building something realistic around food, movement, medications, and monitoring that fits into your real life, not just a pamphlet version of it.
It can, and the hardest part is that you usually will not feel it happening. Diabetic retinopathy builds quietly over years. By the time your vision actually shifts, damage has often already been done. A dilated eye exam every year is the one thing that catches it early enough to make a real difference.
Cold feet, leg cramps while walking, slow-healing wounds, and numbness are early warning signs many people ignore. Poor circulation and nerve damage can lead to serious foot problems.
What a Comprehensive Diabetes Visit Actually Covers
If you are not sure what your diabetes visits should include beyond an HbA1c, here is a practical picture of what a thorough diabetes care plan looks like over the course of the year.
At least once a year your doctor should review your blood pressure, cholesterol, and kidney function. A urine test checking protein is one of the earliest signs that diabetes is beginning to affect the kidneys, and it is easy to miss if no one is looking. A foot exam, checking for sensation, pulses, and skin changes, should also happen at least annually and more often if you have existing circulation or nerve concerns.
An eye exam by an eye doctor who dilates to your pupils should happen every year. Not an eye chart at the clinic. An actual dilated exam.
Dental care matters, too. Diabetes raises the risk of gum disease, and gum disease in turn makes blood sugar harder to control. It is a two-way relationship that most people are not told about.
Vaccinations, particularly flu and pneumonia, are recommended because infections hit harder and take longer to resolve when blood sugar is not well controlled.
The visit itself should feel like a conversation, not a clipboard. At Peoples Medical Care McKinney, Dr. Zulfarah Ishaque and Dr. Munaza Gohar approach every diabetes visit that way. You leave with a clear sense of what is going well, what to watch, and what to do next.


