Nobody sits down one morning expecting to hear the words atrial fibrillation. Usually, it comes up during a visit you booked for something completely different, a blood pressure rechecks, a minor follows up, and suddenly the whole appointment shifts.
What makes it harder is that hypertension and atrial fibrillation have usually been built quietly together for years before anyone catches them. Your blood pressure is creeping up. Your heart compensates in ways you never felt. Once you understand how these two conditions feed each other, everything about managing your health looks different.
Key Take away:
- Uncontrolled blood pressure is one of the leading causes of AFib, and the two conditions actively make each other worse.
- Remote cardiac monitoring catches AFib episodes a standard EKG would completely miss.
- Treatment ranges from rate control medications all the way to catheter ablation depending on where things stand.
- Newer blood thinners for AFib are far easier to manage than older ones and exist specifically to prevent stroke.
- Weight loss, blood pressure control, and treating sleep apnea can genuinely reduce AFib episodes and sometimes eliminate them altogether.
How AFib and Hypertension Work Against You at the Same Time
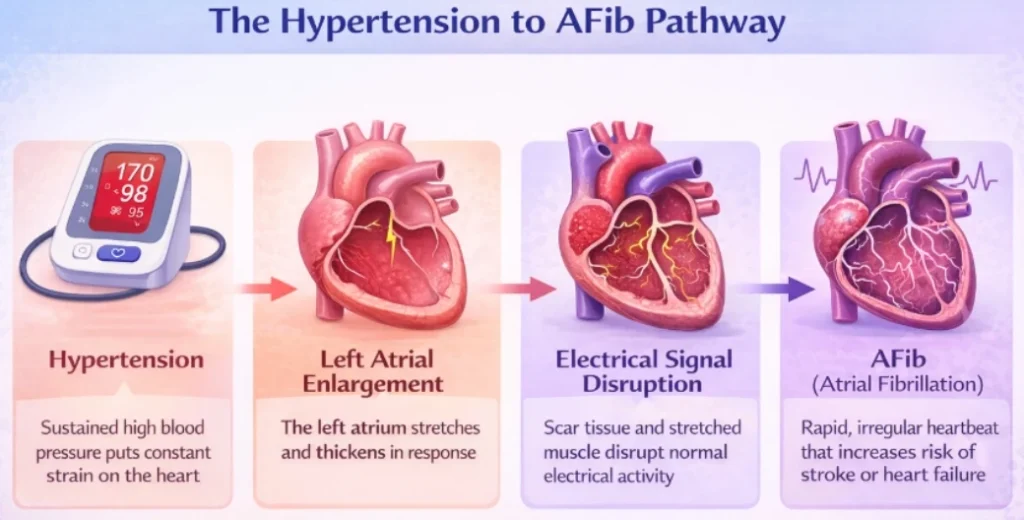
Picture what your heart goes through when blood pressure stays high for months or years. Every beat is pushing against more resistance than it should. The walls are thick. The chambers stretch. The upper left chamber begins to enlarge and stiffen from the constant strain.
That is where things start going wrong. A healthy atrium fires clean, coordinated signals that keep everything steady. One that has been stretched and stiffened from years of high pressure does not work that way anymore. The signals get scattered. The atria start quivering rather than squeezing properly. Blood stops moving through them the way it should.
That quivering is what afib and hypertension look like working against you at the same time. Chronic high pressure also drives inflammation inside blood vessels and gradually rewires how the heart handles electrical stress. That combination of structural damage and inflammation is why people with uncontrolled blood pressure are so much more likely to develop AFib than people whose numbers stay in a healthy range.
The Obesity and AFib Link Nobody Really Talks About
The relationship between obesity and atrial fibrillation is more direct than most people realize. Fat tissue that builds around the heart sits physically adjacent to the atria and affects how that tissue conducts electrical signals. It is not a vague downstream effect. The fat is right next to the tissue responsible for your heart rhythm.
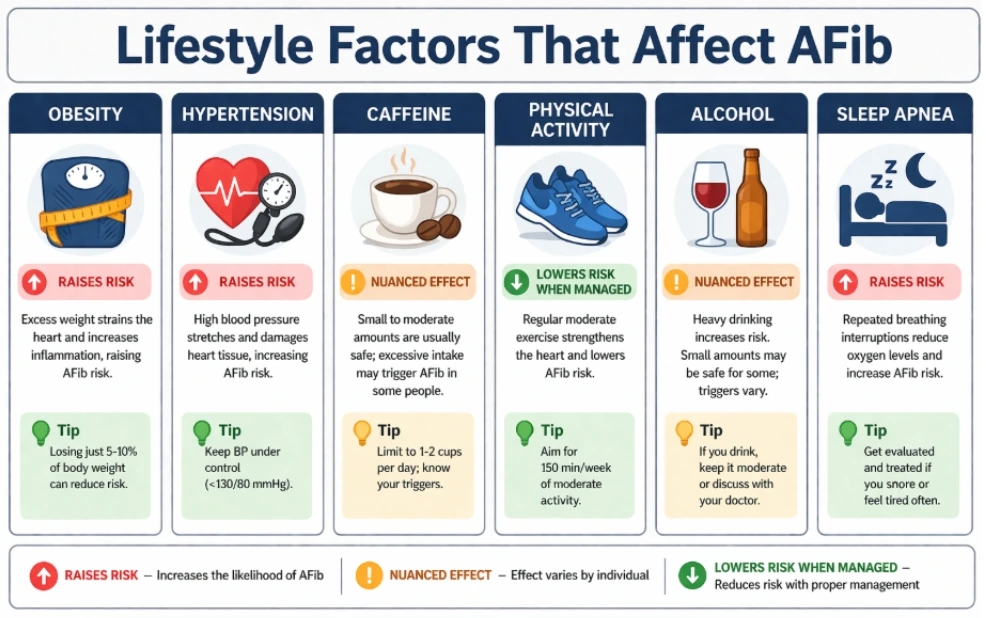
Beyond that, obesity raises blood pressure, makes sleep apnea worse, drives inflammation, and puts mechanical pressure on the heart chambers. Each of those things independently raises AFib risk. When they all show up together, the combined effect is much larger than any one of them alone. Losing even five to ten percent of body weight measurably reduces how often AFib episodes occur in people who already have the condition.
The Symptoms That Are Easy to Explain Away
Both conditions share the same frustrating quality. They can be completely silent for a long time. High blood pressure almost never causes noticeable symptoms until something serious has already happened. AFib for a lot of people is the same way.
When symptoms do appear, they are the kind you talk yourself out of. A fluttery feeling in your chest that lasts a few minutes and stops. Fatigue that makes sense because you have not been sleeping well. Getting breathless during something you do all the time. Some people never feel a thing and only find out because monitoring picked something up during a visit for an unrelated reason.
Two conditions actively raising your stroke and heart failure risk can both run quietly without a single obvious symptom. Anything that feels even slightly off is worth mentioning at your next appointment rather than tucking away on a list of things to watch later.
Remote Cardiac Monitoring and Ambulatory Heart Monitors
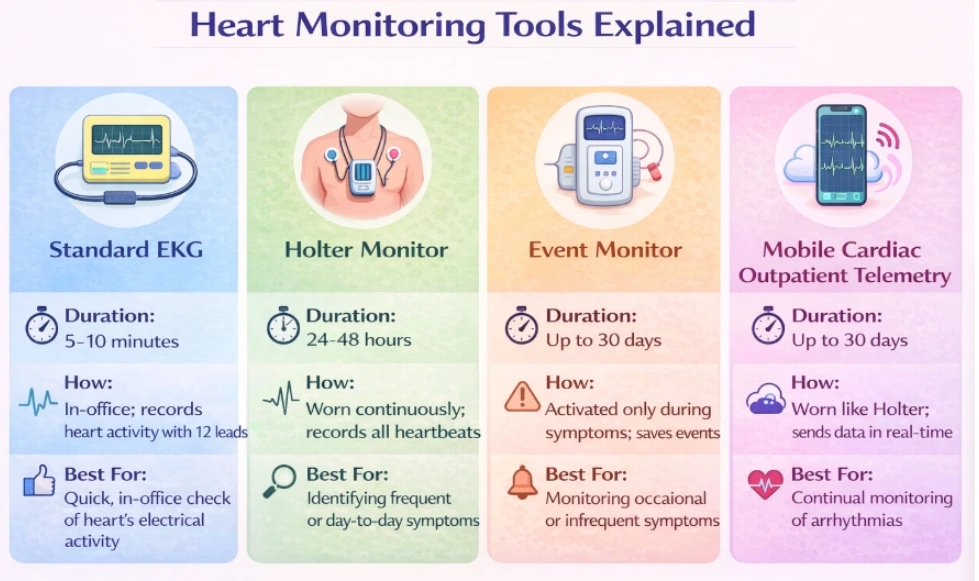
AFib comes and goes. A standard EKG takes a ten second snapshot.Your heart gets to pick when it misbehaves and if it picks a quiet moment during the test everything looks fine on paper. Remote cardiac monitoring exists specifically because that happens more often than most people realize.
An ambulatory heart monitor is a small wearable device you take home and wear through your normal day. A Holter monitor records continuously for 24 to 48 hours. A longer-term event monitor captures episodes over several weeks as they happen. Mobile cardiac outpatient telemetry goes further by transmitting your heart data in real time to a monitoring center where someone reviews it as it comes in. Something abnormal shows up and your care team hears about it right then rather than three days later when a technician finally pulls up the recording.
A heart monitor app for iPhone and similar smartphone tools can also flag rhythm irregularities worth discussing with your doctor. Think of them as a reason to start a conversation rather than a diagnostic tool on their own.
Atrial Fibrillation Treatment Options
Atrial fibrillation treatment options can be matched specifically to what is happening with your heart rather than defaulting to the same approach for everyone.
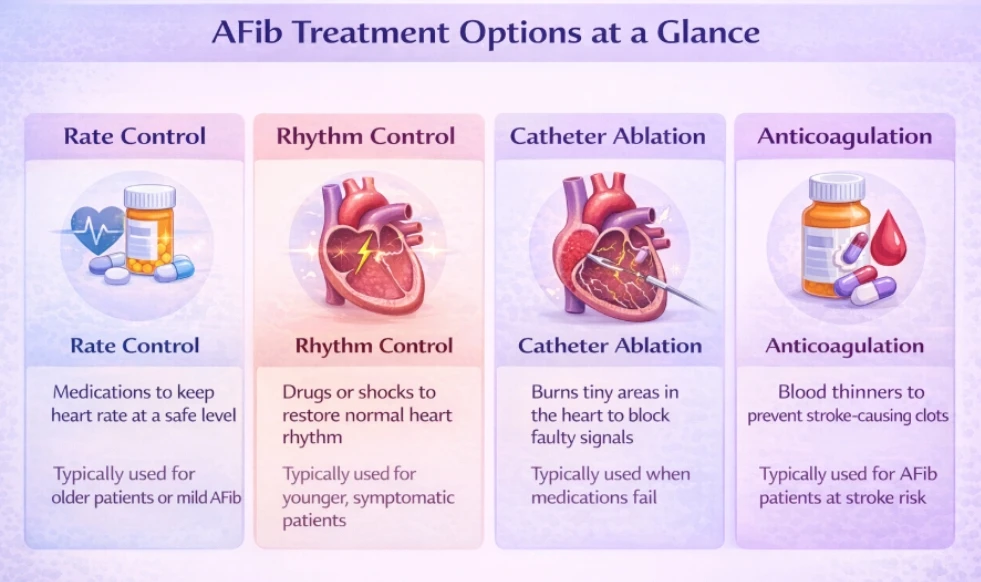
For many patients the starting point is rate control, slowing the ventricular rate even while the atria are still firing irregularly. Beta blockers and calcium channel blockers handle this for most people. Rhythm control goes further and tries to restore a normal coordinated heartbeat through medications for atrial fibrillation or through cardioversion which uses a brief controlled electrical shock to reset the rhythm.
Catheter ablation for AFib is the option people ask the most questions about. A cardiologist uses energy delivered through a thin catheter to destroy the small patches of tissue firing out the irregular signals. Many patients experience meaningful lasting improvements. It is not a guaranteed permanent fix, but for the right candidates it is the most durable form of rhythm control currently available.
Blood Thinners for AFib
When the atria are quivering rather than pumping properly, blood can pool inside them and form clots. If one of those clots travels to the brain, the result is a stroke. Blood thinners for AFib are what stops that chain of events from completing.
Newer medications for atrial fibrillation like apixaban, rivaroxaban, and dabigatran have made this much more manageable than the older warfarin approach. Predictable dosing, no routine monitoring required, and a strong safety record. Blood thinners for AFib are not right for every patient though. Kidney function, bleeding history, and other individual factors all shape which option makes the most sense for your specific situation.
High Blood Pressure and Kidney Damage
High blood pressure and kidney damage work against each other in a loop that keeps getting worse if neither is addressed. Elevated pressure gradually wears down the tiny blood vessels inside the kidneys, reducing their ability to filter waste. As kidney function drops, the kidneys lose their ability to regulate blood pressure, which pushes pressure further.
For anyone managing AFib alongside hypertension, this has real practical consequences. Some anticoagulants and antiarrhythmic drugs are processed through the kidneys so reduced kidney function directly affects which medications are safe at which doses. Keeping blood pressure under control protects your heart and keeps your full range of treatment options available.
Can AFib Be Reversed, Can You Still Exercise, What Else You Need to Know
Can AFib be reversed? The short answer is that it depends entirely on timing and effort. Catching it early gives you a real fighting chance. Patients who got serious about blood pressure, lost weight, addressed sleep apnea, and pulled back on alcohol have seen their episodes shrink significantly or go away completely. For patients who have had AFib longer, the focus shifts toward managing symptoms and preventing stroke. Catheter ablation for AFib remains the strongest option for long term rhythm control in the right candidates.
Can you exercise with AFib? For most people, yes. Staying inactive over time actually makes AFib worse. Light to moderate activity like walking, swimming, or cycling is generally well tolerated and genuinely good for you. A quick conversation with your doctor before ramping up activity is worth having if you have recently been diagnosed.
Caffeine and irregular heartbeat no longer carry the blanket to avoid all coffee recommendations they once made. Moderate caffeine does not appear to reliably trigger AFib in most people. Your own pattern of symptoms is a better guide than a general rule.
Is AFib hereditary? Genetics do play a role. Having a parent or sibling with AFib raises your lifetime risk meaningfully. It does not make AFib inevitable, but it means blood pressure control, weight management, and earlier screening carry more weight in your case.
Is AFib a disability? Not automatically, but it can qualify when episodes are frequent, treatment has not brought adequate control, and functional limitations are clearly documented over time. A physician who knows your full picture is the right person to support that process.
There is no single answer that fits everyone. Some people do well with rate control medications. Others need rhythm control through medication or cardioversion. For the most durable long term result catheter ablation is currently the strongest option. Losing weight, controlling blood pressure, and treating sleep apnea make a real difference alongside any treatment.
AFib comes and goes. A standard EKG only captures ten seconds of your heart’s activity. If your heart behaves during those ten seconds the test looks normal even if something is happening the rest of the time. An ambulatory heart monitor watches what your heart actually does during your normal daily life over hours or weeks rather than one brief snapshot.
Yes and it is one of the most common causes. When blood pressure stays high for a long time the heart’s chambers stretch and stiffen and the electrical signals keeping your rhythm steady start breaking down. Uncontrolled blood pressure over time creates exactly the conditions AFib needs to develop.
Most people with AFib do. When the atria are quivering instead of pumping properly blood can pool and form clots. Blood thinners for AFib exist specifically to stop those clots from reaching the brain.
Remote cardiac monitoring tracks your heart rhythm continuously outside a clinical setting. You wear a small device at home during your normal routine. With mobile cardiac outpatient telemetry that data transmits in real time to a monitoring center so your care team gets alerted immediately if something abnormal shows up.
Managing AFib and Hypertension Starts With the Right Team Behind You
Knowing what hypertension and atrial fibrillation are and how they connect is useful. Having a provider who actively monitors both and builds a real plan around your specific situation is what actually makes the difference.
At Peoples Medical Care McKinney, Dr. Zulfarah Ishaque and Dr. Munaza Gohar manage chronic cardiovascular conditions including hypertension as part of comprehensive primary care. Through the clinic’s affiliation with Southwestern Health Resources, patients have direct access to coordinated cardiology referrals when advanced evaluation is needed.
Book your visit at peoplesmedcare.com or call 469-902-8197. Located at 2001 Auburn Hills Pkwy, Suite 801, McKinney TX 75071. Monday through Friday 8 AM to 5 PM. New patients always welcome.


